GLP-1
A practical 6-week plan for how to avoid nausea on Ozempic
Step-by-step dose timing, meal pairing, and short-term anti-nausea tactics for semaglutide users, with sample schedules and evidence-backed tips.

If your main question is how to avoid nausea on Ozempic, the short answer is to start low, go slow, and use targeted meal and timing tactics while you titrate. Start-low titration combined with meal pairing and short-term antiemetic strategies will usually cut peak symptoms within 2 to 8 weeks. The plan below gives a practical, week-by-week protocol, when to use ondansetron or ginger, and how to time doses around meals to reduce gastrointestinal upset.
What causes the nausea with Ozempic
Understanding mechanism helps you treat it. Semaglutide and other GLP-1 receptor agonists work at both gut and brain receptors to slow gastric emptying and reduce appetite. The slowed gastric emptying produces early satiety and a sense of nausea for many people, especially with higher doses or rapid escalation. A central effect in the area postrema and vagal signaling also contributes to nausea. Two mechanisms explain most cases: slower gut transit and central emetic signaling. See the clinical review on GLP-1 gastrointestinal effects for more detail NCBI review.
Timing matters because the body adapts. When you start Ozempic or increase the dose, that sudden increase in receptor activation causes a transient rise in nausea risk. Over several weeks the gut and central pathways desensitize for most people. In the STEP and other semaglutide trials those early weeks were where adverse events clustered, which is why published protocols use stepwise dose escalation to blunt that peak reaction. See the STEP-1 trial results for nausea incidence NEJM STEP-1.
How bad is the nausea, and what to expect
Expect a spectrum. Some patients have mild queasiness for a few days, others have repeated episodes that interfere with work or sleep. In large trials, mild-to-moderate nausea was common, severe events less so. For most people the worst window is the first 2 to 8 weeks after initiation or a dose jump. Use that timeframe to plan protective measures and avoid abrupt increases.
- Typical onset: 24, 72 hours after a dose change for many patients, sometimes sooner with higher-fat meals.
- Peak severity: first 2, 8 weeks after starting or dose escalation, then usually declines.
- When to worry: persistent vomiting, dehydration, or weight loss beyond the intended effect requires medical review.
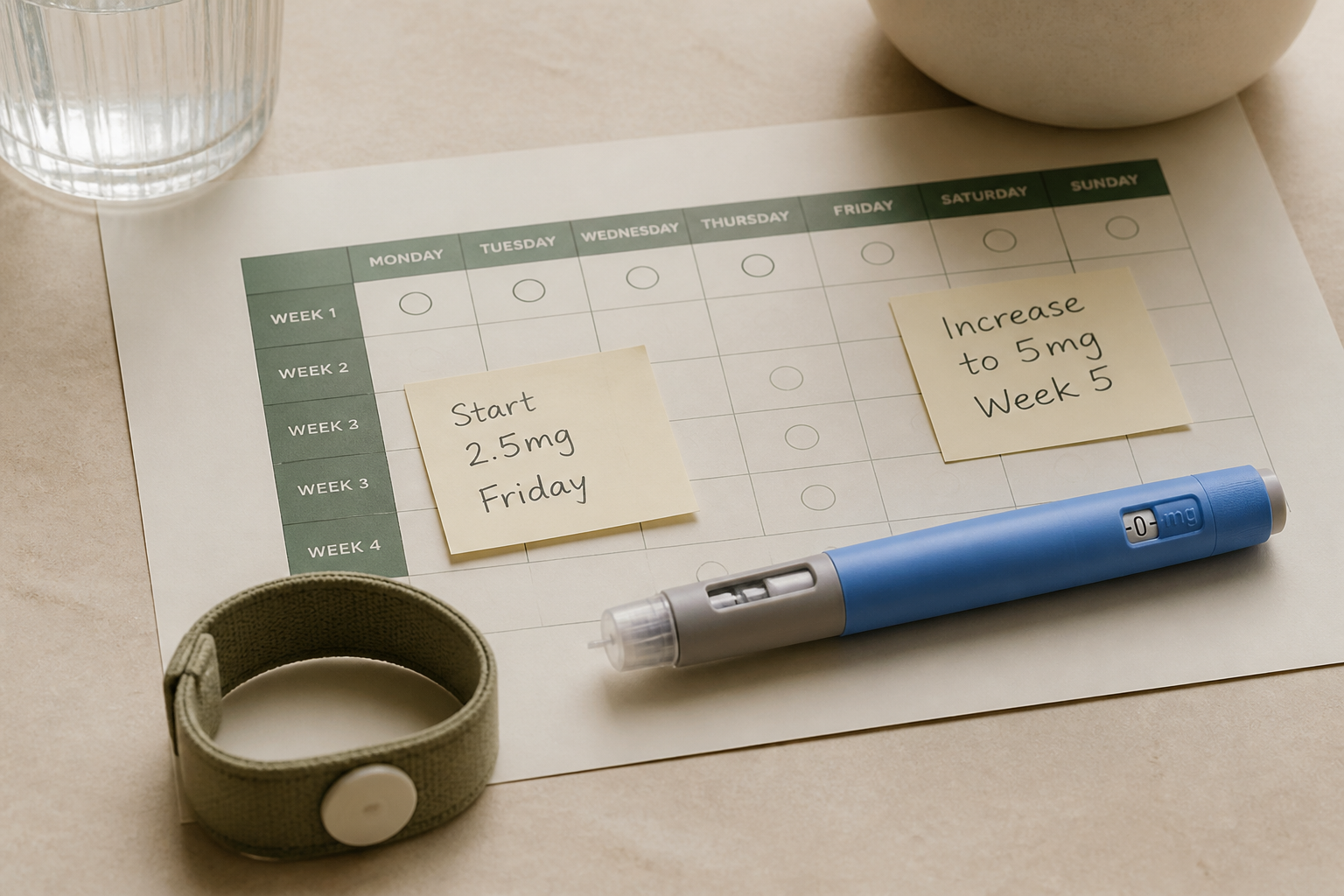
6-week protocol: exact dosing, timing, and food strategy
Below is a practical, conservative plan I use in clinic for people asking how to avoid nausea on Ozempic. It assumes you're starting Ozempic for type 2 diabetes or off-label weight loss and you are not on interacting medications like high-dose insulin or a sulfonylurea without plan for adjustment. Safety first: coordinate with your prescriber if you have complex comorbidities or are pregnant.
The core rules are simple and repeatable: start low, space increases, and pair doses with small meals for two weeks after any increase. For illustration I give a conservative schedule below and a slightly accelerated option for people with close monitoring.
- Week 0 to 4, standard start: inject 0.25 mg weekly for 4 weeks. This is the manufacturer starting dose for Ozempic and designed to ease GI side effects.
- Week 5 to 8: increase to 0.5 mg weekly (or remain at 0.25 mg if symptoms persist). Keep dose increases only after 4 full weeks at the prior dose.
- After week 8: consider moving to 1.0 mg weekly only if tolerated and clinically indicated. Pause escalation if nausea returns or worsens.
If your provider uses a faster titration, use extra food and anti-nausea measures during each step. The goal is to avoid dose jumps after day-to-day poor tolerance; short delays in escalation are usually safer than pushing up and triggering repeated nausea.
When to take your weekly dose
Injection timing is flexible, but timing can reduce symptoms. Injecting semaglutide the same day each week matters for steady-state, but the time of day affects how the first 48 hours of receptor activation overlay with your meals. Many patients report less immediate nausea if they inject after a small meal rather than before a large meal or on an empty stomach. Practically, pick a weekly slot you can pair with a low-fat snack or small meal.
- Evening injection option: after dinner small low-fat snack reduces daytime queasiness for some people, and overnight adaptation often blunt morning symptoms.
- Morning injection option: after breakfast with protein and carbohydrate if evenings are busy or you have morning nausea triggers.
- Consistency is key: pick the same weekday and similar time each week for steady-state.
If you have severe morning sickness after dosing, switch to after your largest meal or to an evening slot. Personalize by tracking which timing reduces your peak symptoms over two doses.

Practical meal and food pairing rules
Food choice matters more than people expect. Because gastric emptying is slowed, high-fat or very large meals prolong gastric fullness and can amplify nausea. The principles: smaller volumes, lower fat, modest protein, and regular timing. Use food to blunt acute queasiness in the first 48 to 72 hours after any dose change.
- First 48, 72 hours after a dose change: 3, 4 small meals (200, 300 kcal each) instead of two large meals.
- Avoid heavy fats: fried foods and high-fat restaurant meals increase nausea risk for many patients.
- Include gentle anti-nausea foods: ginger tea, plain crackers, bananas, plain yogurt, and dry toast.
A sample day to reduce nausea looks like this: breakfast plain Greek yogurt with banana at 7:30 am, mid-morning dry toast at 10:30 am, lunch small chicken and rice bowl at 1:00 pm, and light dinner at 6:00 pm. Keep fluids steady: sipping water or weak ginger tea helps. frankly, the boring meals work best when you're adapting.
Non-drug tools that actually move the needle
Before adding medications, try evidence-friendly non-drug measures. Ginger has randomized evidence for chemotherapy and pregnancy nausea and helps some GLP-1 users by motility and central effects. Acupressure at P6, plain crackers, and avoiding lying flat for 30 minutes after eating can reduce symptoms. These interventions are low-risk and worth trying first.
- Ginger: 500, 1000 mg total daily as tea, chews, or capsules in divided doses for short-term use.
- Acupressure: P6 wrist bands used before and after a dose may reduce nausea.
- Behavioral: slow eating, small bites, and sitting upright for 30 minutes after meals.
Short-term medications: when to use them and which ones
If non-drug measures fail, short-term antiemetics are appropriate. Ondansetron is commonly effective for chemo-related nausea and works for GLP-1 induced nausea in many cases. A typical regimen is ondansetron 4, 8 mg by mouth as needed, up to twice daily for a few days around a dose increase. Coordinate use with your prescriber because of possible QT interactions and other risks.
Other options include dopamine antagonists like prochlorperazine or metoclopramide, but those carry movement-related and long-term risks, so reserve them for short courses and under supervision. For refractory cases some clinicians use low-dose mirtazapine for appetite/nausea, but that is not first-line and requires psychiatric oversight. Start with ondansetron when available and safe for you.
- First-line short-term med: ondansetron 4, 8 mg PRN for 48, 72 hours around a dose change.
- Second-line: prochlorperazine 5, 10 mg every 6, 8 hours PRN, short courses only.
- Avoid chronic metoclopramide use: risk of tardive dyskinesia limits long-term use.
A note on insulin, sulfonylureas, and hypoglycemia risk
If you are on background insulin or a sulfonylurea, nausea plus reduced oral intake can increase hypoglycemia risk. Because Ozempic lowers appetite and caloric intake, coordinate with your diabetes team. Practical steps: lower mealtime insulin or sulfonylurea dose by 10, 30% during the first 2, 4 weeks, and monitor glucose more closely. Prevention of low blood sugar is as important as preventing nausea.
Chart: nausea incidence estimates across GLP-1 agents
Values are illustrative ranges based on STEP, SURMOUNT, and other trial reports; see NEJM STEP-1 and product labels for exact figures.
These bars are estimates based on pooled trial reports. They show that nausea is common with active GLP-1 therapy but not universal, and that dose is a major driver of symptom frequency and severity. See the STEP-1 trial for data on semaglutide dosing and GI events NEJM STEP-1.
Comparison table: dosing and escalation (practical reference)
| Product | Common start dose | Typical escalation | Key nausea advice |
|---|---|---|---|
| *Ozempic* (semaglutide) | 0.25 mg weekly | Increase to 0.5 mg at 4 weeks, then 1.0 mg at 4+ weeks | Start low, pair dose with small meal, use ondansetron PRN |
| *Wegovy* (semaglutide 2.4 mg) | 0.25 mg weekly | 6-step escalation over 16, 20 weeks to 2.4 mg | Longer, slower titration recommended to reduce nausea |
| *Tirzepatide* (dual GIP/GLP-1) | 2.5 mg weekly | Increase to 5 mg after 4 weeks, then 7.5, 15 mg | Similar GI profile; slow escalation and food rules apply |
Note the longer titration with weight-loss formulations like Wegovy reflects the higher target dose and higher rates of initial GI side effects if accelerated. Long titration reduces peak symptoms for many patients.
Troubleshooting common patterns
You will see a few patterns in clinic. Identifying which pattern lets you apply the right fix. Pattern identification is often the fastest route to symptom control.
- Pattern A: early, mild nausea that improves in 3, 7 days. Workup: use ginger, small meals, and ondansetron PRN; continue the current dose.
- Pattern B: recurrent nausea after each dose with partial recovery. Workup: slow titration, change dosing time, consider 48, 72 hours of ondansetron around each injection.
- Pattern C: persistent vomiting or weight loss >5% in first month. Workup: stop escalation, rehydrate, evaluate for alternative causes, contact your prescriber urgently.
"Start low and plan for small, bland meals for the first month. If nausea prevents adequate intake, pause escalation and treat symptoms aggressively."
— Samuel K., MD, functional medicine clinician
not clickbait, the single best immediate move when nausea starts is to go to small frequent meals and try a single antiemetic dose. That combination often prevents escalation without needing to stop therapy. Quick action reduces the chance you'll need to stop treatment entirely.
When to consider dose delay, dose reduction, or stopping
Stopping is a last resort. Most nausea resolves with conservative management. Consider delay or reduction if nausea prevents calorie intake, causes dehydration, or is accompanied by intolerable vomiting. In such cases, revert to the prior tolerated dose for 2, 4 weeks, use antiemetics, then retitrate more slowly. Permanent discontinuation is for persistent severe events or patient preference.
If you have repeated significant nausea after multiple attempts at retitration, switching agents within the GLP-1 class sometimes helps, but cross-reactivity is common. Discuss options with your clinician. Switching is a reasonable pathway when side effects are unacceptable and benefits don't outweigh harms.
Real-world examples and a sample calendar
Here are two anonymized, realistic examples I use with patients when teaching the protocol. Each one illustrates a different tolerance pattern and the action steps.
- Case 1, steady improver: Week 1 start 0.25 mg on Monday evening after dinner; mild nausea day 2 only, managed with ginger tea and crackers. Stayed at 0.25 mg for 4 weeks, increased to 0.5 mg with only 48 hours of mild nausea controlled by ondansetron 4 mg PRN. Continued to 1.0 mg at week 12 without major issues. Outcome: continued therapy with manageable side effects.
- Case 2, sensitive to changes: Week 1 start 0.25 mg with morning dosing after breakfast; persistent mild nausea for 10 days. Provider delayed escalation and added ondansetron 4 mg twice daily for 5 days while switching to evening dosing after small dinner. Symptoms improved, patient remained at 0.25 mg for 8 weeks before slowly increasing. Outcome: avoided stopping therapy by pausing escalation.
A quick checklist to use on dose day
- Before injecting: eat a small low-fat meal (yogurt and banana or toast) within 30, 60 minutes.
- Have ginger or crackers at hand: prepared anti-nausea food reduces panic if symptoms begin.
- Have an antiemetic option discussed with your clinician: ondansetron plan if needed for 48, 72 hours.
Evidence and practical caveats
Clinical trials like STEP demonstrated meaningful weight loss and glycemic benefits with semaglutide but also higher GI-related adverse events in active arms. Trial data show nausea clusters early and declines over time in many participants. Real-world experience mirrors that, and most strategies recommended here are supported by mechanistic understanding and clinical practice rather than large randomized anti-nausea trials specifically in GLP-1 users.
If you're interested in the data, the manufacturer label and trial publications report the incidence and timing of nausea. For practical guidance the Mayo Clinic and Cleveland Clinic pages summarize side effects and monitoring advice, which I reference when I plan patient follow-up Mayo Clinic semaglutide and Cleveland Clinic summary. Use them as starter references.
Key takeaways
The takeaways
- Start with 0.25 mg weekly and give your body 4 weeks at each step when possible to reduce nausea.
- Pair weekly injections with a small low-fat meal and keep meals small and frequent for 48, 72 hours after dose changes.
- Use short-term ondansetron 4, 8 mg or ginger for 48, 72 hours around dose increases if non-drug measures fail.
- Delay escalation rather than stopping if nausea is significant; revert to the prior tolerated dose and retitrate slowly.
- Coordinate with your diabetes team if you are on insulin or sulfonylureas to prevent hypoglycemia during adaptation.
Common questions
Below are brief transitions and common questions I hear; the detailed answers follow in the FAQ section. Read these if you want quick, actionable answers about dose timing, antiemetics, and when to call your clinician.
Sources & further reading

About the writer
Senior Staff Researcher
Elena leads background research for the PuraGene Journal. She spends her days digging through peer-reviewed studies, product monographs, and trial data so the rest of the team has something honest to work from. She is not a clinician and does not give medical advice. she reads the studies and writes up what they actually say. Based in Austin.
Frequently asked
- How quickly should I expect nausea to improve after starting Ozempic?
- Most people see improvement in 2, 8 weeks after starting Ozempic as the body adapts. Initial nausea often peaks in the first 48, 72 hours after a dose change, and with conservative titration and dietary measures the intense phase usually lasts less than a week. If nausea persists beyond 2 to 4 weeks without improvement, contact your provider for a reassessment.
- Should I take Ozempic in the morning or evening to reduce nausea?
- There is no universal rule, but many patients do better when they inject after a small meal rather than on an empty stomach. If morning dosing causes symptoms, try moving the weekly injection to after dinner for a couple of doses to see if overnight adaptation reduces morning queasiness. The most important factor is consistency in timing.
- Can I use ondansetron with Ozempic, and what dose works?
- Yes, short courses of ondansetron 4, 8 mg can be used PRN for GLP-1 induced nausea, typically for 48, 72 hours around a dose increase. Discuss with your prescriber first because ondansetron can interact with other meds and has QT considerations. Use the lowest effective dose for the shortest time necessary.
- Are natural remedies like ginger effective?
- Ginger is a reasonable first-line option and has clinical evidence in other nausea contexts. Use 500, 1000 mg daily divided or ginger tea and see if symptoms abate. It's low-risk and often helpful when combined with small, bland meals and acupressure.
- When should I stop Ozempic because of nausea?
- Consider stopping only if nausea causes persistent vomiting, dehydration, unintended rapid weight loss, or interferes with daily life despite conservative measures. More commonly, pausing escalation and using short-term antiemetics allows continued therapy. Always consult your prescriber before stopping.
- Will switching to another GLP-1 solve my nausea problems?
- Sometimes changing agents or choosing a slower titration schedule for a different formulation helps, but cross-reactivity of nausea across GLP-1 drugs is common. Switching is an option after failed retitration but should be done with prescriber oversight.
- How should I adjust insulin or sulfonylurea doses when starting Ozempic?
- Reduce mealtime insulin or sulfonylurea doses by 10, 30% initially and monitor glucose more intensively during the first 2, 4 weeks. Since Ozempic reduces appetite and caloric intake, hypoglycemia risk increases. Coordinate exact adjustments with your diabetes clinician.
- Are there long-term strategies to prevent nausea if I plan to stay on Ozempic?
- Yes: maintain stable dosing once tolerated, plan meals with low fat and moderate protein, avoid rapid dose jumps even later on, and keep short antiemetic options available for any future dose increases. Long-term habituation commonly reduces nausea intensity over months.